being large variety productions from different manufacturers, besides Siemens Lithostar, EDAP LT.01 and Sonolith 2000, Sonolith 3000 Versions.[48,49]
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
Extracorporeal shock wave lithotripsy, and its role in urolithiasis, with emphasis on lower pole, inferior calyx kidney stones, lower ureteric, Vesico-Ureteric Junction stones,
and gall stone diseases
Dr.Anil K. Sahni M.S, F.I.C.S, Advanced D.H.A Surgeon, Medical Teacher
than 95% success rate, while single sitting clearance achieved in about ≥50% cases.
Conclusions:For all practical purposes, renal and ureteric calculi can be treated with ESWL with almost cent percent (complete) success, up to a solitary stone size of 45 mm, with/without supportive measures, excluding various limiting conditions
1.INTRODUCTION
Successfully acceptable management modality of urolithiasis, with extendable scope for other stone
diseases. [1,2] Extra corporeal shock wave lithotripsy (ESWL), being convenient noninvasive, safely performed OPD
A patient undergoes the procedure in the morning
discharged in the afternoon, and can go to day-to-day work by the next day with advice for follow-up.
--------------------------------------------------------------------------------
Auth o r’s Corre spo nde nce Addre ss:
Dr.Anil K.Sahni
A-1 / F-1 Block-A Dilshad Garden Delhi-110095 India.
E-Mail:dranil_sahni@yahoo.co.in dranil_sahni@hotmail.com
Besides controversially successful various medical therapy
regimes, and OSS (classical open surgical stone extraction),[3] other methods include: (1) Percutaneous nephrolithotomy(PCNL) for renal calculi, (2) Retrograde ureterorenoscopic Intrarenal surgery, (3) Ureterorenoscopy (URS) and Lithoclastfor ureteric calculi, (4) Laparoscopic ureterolithotomy,(5) Cystolithopexy/Cystolithoclast for vesical calculi,using Lithotrite, (6) Sandwich technique (ESWL + PNL/Ureterorenoscopic Lithotripsy surgery), etc.
[5-7]
HISTORICAL ASPECTS:
Urolithiasis Management has undergone drastic changes
since early 1980s, with popularization of endourology, ESWL, and PCNL techniques. High-energy shock waves
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
have been recognized for many years, Beginning 1969, Dornier (German Ministry of Defense) reported studies of shock wave effects on tissue. However, the production and distribution, Dornier HM3 lithotripter availability, began late in 1983, whereas US Food and Drug Administration approval for ESWL obtained in 1984.
Since then, numerous companies came with different models, using various technical know-how and varying efficacies, lithotripters.
EXTRA SHOCK WAVE LITHOTRIPSY;
METHODOLOGY & BIO-PHYSICS:
Shock waves produced by a source, outside a patient body,
are propagated inside the body focused on stone. Externally generated relatively weak nonintrusive waves, transmitted through the body, building sufficient strength at the target site to break stone, are achieved by uniqueness of this device. Rapid energy deposition into fluid leads to shock wave production invariably. This is described as surfaces, dividing material ahead, not yet affected by the disturbance at the source from material behind, which has been compressed as
a consequence of the energy input (Sturtevant, 1996). With
the behavioral characteristic of propagation of nonlinear waves moving faster than the speed of sound, shock waves’ speed is in direct proportion to the shock strength.[50] GENERATOR TYPES
in water containing hemi-ellipsoid reflector, separated
from patients body by an insulated membrane, spherically expanding shock waves coherent to calculus, achieved by placement of focus (F1) electrodes in ellipsoid, with the target stone at other focus (F2). Have clear Advantage of effectiveness, Disadvantages include substantial pressure fluctuations from shock to shock and relatively short electrode life.
by a parabolic reflector, are transformed into spherical waves. In a water field, a shock tube containing two cylindrical
places separated by a thin insulating sheet, electrical current through one or both conductors, resultant strong magnetic field, electromagnetic force, termed magnetic pressure producing under water pressure shock waves, Made target specific coherence, is utilized for stone fragmentation. Advantages Over The Electrohydraulic Generator:
(1) due to no ‚variable‛ in the design, e.g., under water spark
discharge, electromagnetic generators are more controllable
and repeatable;
(2) energy entrance involving a large body surface area, through patients, rendering EMG less painful. Disadvantages include a small focal region of high energy resulting in an increased subcapsular hematoma formation rate in modified E.M.Gs
ceramic elements produced plane shock waves with directly converging shock fronts, used for stone fragmentation. Advantages include accuracy, durability, and less painful
anesthetic free treatment due to low energy density at
insufficient power delivery for stone fragmentation.
With Intra-Corporeal Appliances: Produced Shock Waves Are
Utilized Within Patients’ Body Directly To Stones.
Stone Fragmentation Biomechanics
1. Electrohydraulic lithotripsy: Cavitation bubble formation mechanism.
2. Laser lithotripsy: Plasma bubble formation, shock wave mechanism, holmium: Yag Laser (yttrium–aluminum– garnet), Erbium: YAG
3. Ultrasonic lithotripsy: By ultrasound vibrations
4. Ballistic lithotripsy: Projectile movement, Jackhammer effect mechanisms.
Potential Mechanisms For ESWL Stone Breakage: Explained by typical pressure pulse, tensile pressure (positive and negative phase), reversed pressure theories;
(1) Compression fracture, (2) Spallation,
(3) Acoustic cavitations and Bubble formation,
(4) Dynamic fracture fatigue,
Cumulative damage accumulation during course-off treatment leading to eventual stone destruction.
2.MATERIALS AND METHODS
This study comprises more than 300 patients of renal, ureteric calculi, including gall-stone disease, that were completely removed by ESWL(Personally Performed), with an average of about two sittings.
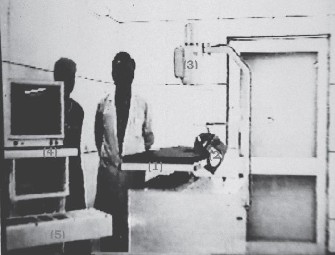
STONE-LITH(PCK) LITHOTRIPTER
Various studies involving several aspects for lithotripter
comparisons are available. Despite claims to the contrary, unmodified HM 3 Dornier lithotripter remains the gold standard for ESWL, others included for comparative trials
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
being large variety productions from different manufacturers, besides Siemens Lithostar, EDAP LT.01 and Sonolith 2000, Sonolith 3000 Versions.[48,49]
Figure 1: Stone-Lith (PCK) Litho-Triptor
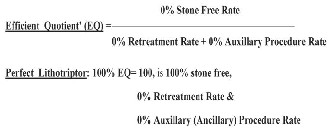
Figure 2: lithotriptor efficient quotient (EQ) TECHNIQUE
disease excluding distal obstruction, ensured patient compliance after comprehensive awareness of a treatment plan, needed ureteral stenting, urinary asepsis, etc. Avoidance or restriction of aspirin-containing
products(as monitored by BT,CT,INR etc), nonsteroidal
anti-inflammatory medications, besides exclusion and/ or management of pre-existing illnesses are required. Preprocedural preparations including overnight fasting, bowel preparation, immediate bladder evacuation etc are needed.
(a) Patient stone side toward the machine,
(b)Lies supine, for renal and upper, mid,ureteric calculi, and
(c) Prone position, for lower ureteric/VUJ stones.
(subcostal region, umblicus, ASIS, pubis and other bony points pelvis, vertebrae), maneuvering table movements
and may be assisted by patient movement as a whole.
1ml Pentazocine (Fortwin) (+) 2 ml (Phenargan)
promethazine, diluted to 5 ml by adding 2 ml distilled
water, 3 ml of preparation given slowly intravenously, and remaining 2 ml given intramuscularly, achieves almost complete sedation and analgesia for conducting lithotripsy sitting for about 100 min.
patient’s social history (previous painkiller injections,
smoking, alcohol etc.) and associated medical problems.
(b)Vital signs, especially pulse respiration etc
(c) Regulation shock mode, power, and frequency; while maintaining patient’s compliance throughout are the key components
for the complete stone-free success rate.
or forced diuresis, as indicated.
Urinary antiseptics according to C and S, prophylactic antibiotics, analgesia and other supportive therapy.[8]
Advice to filter all urine and collect stone particles.
FUCs, as advised, for next sitting or otherwise [Figure 3]
3.DISCUSSION
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
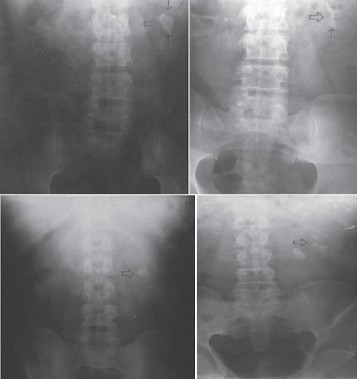
Figure 3: Screening Stages For Subsequent Complete
Removal Left Renal Stone About More Than 3 Cms
stone formation by stasis, are indication for surgical exploration of stone, and simultaneous correction of defect and/or associated management.
Advantages (lithotripsy):
(1) Noninvasive,
(2) Usually done as OPD procedure,
(3) Patient resumes routine work within 24 h and is stone free
within 1-to-2-month time,
(4) Avoiding hazards of anesthesia and surgical procedures in patients not willing for and/or unfit for such extensive procedures.
ROLE OF D OUB LE ‘J’ STEN T
or management need for pre-existing illnesses.
However, in large, hyperdensity stones, double J stenting may be of great importance preventing obstructive processes like ‚Stone/Steine Strasse.‛[24-26] Indications Include:
(1) Obstructive uropathy duration,
(2) Associated infection, (3) DTPA renal scan, with/without
diuresis or other indices, revealing decreased renal function.
UROLITHIASIS MEDICAL THERAPY REGIMES: (I)FORCED DIURESIS(LASIX THERAPY);
Done for stones Size up to 5-8 mm, remnant post-ESWL stones. Recommended ideal forced diuresis regimen: Complete compliance achievement ensures promising good results.
5% DNS ≈ 1,500 ml (3 vacs)
(+) R/L ≈ 1,500 ml (3 vacs) (Alternating) In 24 hours Repeat for 3 days.
Inj. Lasix 1 amp. Im, after (II) and (IV) Vac
(regular BP monitoring).
The role of injection Drotaverine (Drotin), Hyoscine (Buscopan), Diclofenac (Voveran) Bd/Tds, is to achieve round the clock analgesia and spasmolytic effect, as needed.
4 days. The patient encouraged for high fluid intake with normal diet, to ensure about >1.5 to 2 litres/24 h urine output. Straining of all urine is done to filter passed stone
particles (Stone analysis sampling). (II)MEDICATIONS;Commonly used preparations: Zyloric (Allopurinol)––for Uricemia (S. uric acid ≥7 mg%) decreases S. uric acid and thus disintegrating uric acid (invisible) component of stones, Various Other Ayurvedic Preparations: Cystone, Neeri, Distone, Calcury, Smash, Expel, Nephrol Etc.
& Commonly Available Urinary alkalizers.
STONE ANALYSIS
techniques, provides guidelines for dietary regulation and subsequent management for stone disease, especially for recurrence.[23]The composition Studies reveal either of the following ingredients: Calcium oxalate monohydrate stone, Calcium oxalate Dihydrate stone, Uric acid stone, Cysteine stone, Purine stone, Hydroxyapatite stone, Carbonate stone, Struvite stone (infection), and Others, e.g., soft radiolucent stone ‚Indinavir‛(a Protease inhibitor) and stone formed during Aids treatment, etc.[21,22]
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
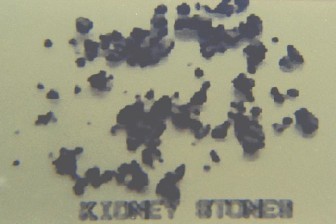
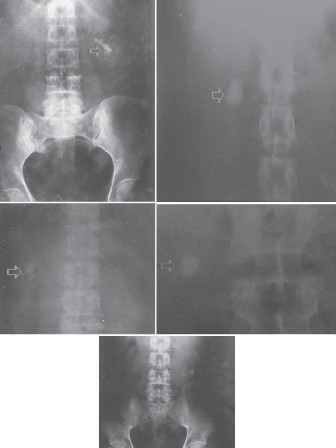
Figure 4: Fragmented Stone Particles Passed With Urine The Various Constituents, alone or in varying proportions/ percentages, provide directive for comprehensive management, guidelines for stone disease.
DIETARY REGULATION
According to stone composition and availability of food products, various scientifically approved diet regulation regimes are available by different laboratories and pharmaceutical companies, especially Restricting oxalate, calcium, urate, and other mineral-containing food items, while Promoting intake of food substances with ingredient content known to be effectively helpful for stone disease.
METABOLIC EVALUATION
Consideration of metabolic evaluation of patients with stone
disease provides useful Diagnostic and/or Therapeutic tool
for medical and surgical management guidelines, more so
in recurrence cases.
SUPPORTIVE MANAGEMENT EMPHASIS: INFERIOR CALYCEAL STONES,
LOWER POLE KIDNEY STONES [11]
Choice of patients, anatomical and/or other determinants,
consideration and Postprocedural Period Advice;
had synergistic result outcome effects.[14,16-18]
Figure 5: Kidney And Ureteric Stones Of Different Sizes, Locations(LPS Etc.) Removed Completely
LOWER URETERIC STONES
Being technically difficult eitherwise, have comparatively
low success rate usually, and are less attempted by lithotripsy. However, ESWL gives good result yield, and not uncommonly
performed in patients demanding specific treatment modality, reluctance, or contraindication for surgery.
supportive measure, minimizing the use of ‘DJS’, avoiding
obstructive phenomenon, e.g., stein-a-strasse, by expelling out minutely shattered stone particles.[12,13]
ROLE IN GALL STONE DISEASES
T-tube drainage or otherwise, Contrast Delineated Stones
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
![]()

R ENAL A NAT OMY‛ P R EDI CTIVE FACT OR S‛ /
‚ DETER MINA NTS‛
anomalies, Hydronephrosis, and Calyceal diverticulae[9,10]
In cases of ureteropelvic junction obstruction, in addition to anatomic obstruction, coexistent metabolic abnormalities
are contributing to stone formation.[4] Suggestive
Treatments for PUJ obstruction with stone; classical
open surgical stone extraction and pyeloplasty, PNL with concomitant endopyelotomy, and recently laparoscopically (an antegrade approach preferred with existing stone, although retrograde can be performed) [Figure 6].
Treatments include traditional open surgical nephrostomy with infundibulum closure and diverticular cavity fulguration, invasive surgical PNL ureteroscopy, ESWL, and laparoscopy.
Reported Stone free rate for calyceal diverticular stone
treatment with ESWL averages only 21%.
Inferior Calyceal Stones: Can Be Managed EitherWise Or By ESWL, As Discussed With The Special Emphasis Supportive Measures & MethodologyTechnique.
[32-34]
• Lower Pole Infundibulopelvic Angle (LIP): Lower border of pelvis with the medial border of lower pole infundibulum is equal to or more than 70–90°.[30,35]
• Ureteropelvic Axis: Central point of renal pelvis and central point of the proximal ureter.
• Diameter Of Infundibulum (IW): More than 4–5 mm.
• Infundibulopelvic Length (IL): < 3 cm.
• Spatial Distribution Of Calyces, Distorted Calyces System
Figure 6: IVP Films –
Kidney, Renalpelvis Stone About 1.5 Cms
Subsequent IVPs After About > 6 Months:WNL, Single Sitting Clearance.
AGE RELATED CHANGES
IN ESWL ‘R ESISTIV E -IN DE X’ .[31]
1. Presence of distal obstructions: Obstructive uropathy, urolithiasis, hydronephrosis; poor results of ESWL, and other important reasons for residual fragments,
2. Febrile urinary tract obstruction,
3. Distal calculi in females,
4. Morbid obesity (more than 100 pounds): However, the patient body weight limit for Dorniers H3 Lithotripter is about 280 pounds.
5. Other associated anatomico functional problems: Spinal deformity, limb contractures, etc.
CONTRAINDICATIONS:
1. Pregnancy (only absolute contraindication)For LithoTripsy,
2. Uncontrolled coagulation disorders,
3. Uncontrolled hypertension: Relative renal hypertension.
COMPLICATIONS
good result besides other supportive measures including cause evaluation and management.
Intra-Parenchymal of varying severity.
Need Increased caution In Bleeding––Diasthesis, hemophilia,
polycystic (autosomal dominant) kidney disease, hydronephrosis etc.[37]
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
etc.[41-43] Routine urine test for crystalluria, sediments, and
casts provides useful index besides various metabolic evaluators. [44]
renin activity phenomenon and other factors, various study reports are available.[38,39,40]
BJU International (2001) reported.
accumulation of stone fragments obstructing ureter after ESWL being 2–10%, large stone burden staghorn calculi, bilateral ESWL, pre-existing ureteral obstruction are known risk factors [Figure 7A and B].[27,28]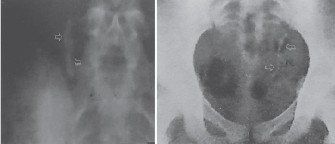
Figure 7: (A)Stone particles passage Rt. Mid ureter
P he nom e no n Kno wn As ‚ Stone / St e ine Stra sse ‛
Pre-ESWL Ureteral Stenting Significantly Decreases But Do Not Eliminate Steinstrasse (Controversial Reports). Spontaneous stone clearance occurs in 60–80% cases; failure to resolve within 3–4 weeks time, with special indications for bilateral obstruction, solitary kidney, severe refractory pain or infected hydronephrosis,
Necessitates intervention aiming prompt urinary track decompression by ureteral stenting, nephrostomy tube drainage, URS management including basket extraction etc.
ESWL aimed for fragmentation of steinstrasse has a high success rate with minimal complications.
4.RESULTS
used in about 15–20% cases; improved results outcome was achieved by reducing number of sittings in large kidney and
ureteric stones, while improved overall treatment efficacy in LPS, inf. calyceal, lower ureteric, especially VUJ stones, residual stone fragments and also as an adjunct to medical therapy, achieved in selected cases.
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
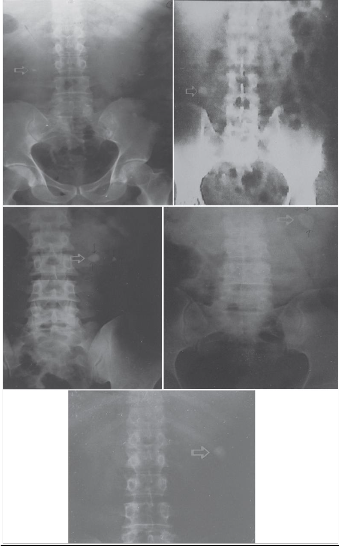
Figure 8: Kidney And Ureteric Stones Of Different Sizes, Location, Completely Removed
4.CONCLUSIONS
5. REFERENCES
1994;45:218-21.
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
Urol 1988;14:414-6.
1990;144:15.
9. Küpeli B, Isen K, Biri H, Sinik Z, Alkibay T, Karaoğlan U, et al. Extracorporeal shock wave lithotripsy in anomalous kidney. J Endourol 1999;13:349-52.
lithotripsy for lower pole nephrolithiasis: Efficacy and variable
that influence treatmentoutcome. Urology 1998;51:544-7.
1989;142:774-7.
15. Küpeli B, Biri H, Sinik Z, Karaca K, Tuncayengin A, Karaoğlan U, et al.Extracorporeal shock wave lithotripsy for lower calyceal calculi. Eur Urol 1998;34:203-6.
1991;146:953-4.
J Urol 2001;166:2065-71.
J Urol 1989;142:774-7.
19. Küpeli B, Biri H, Sinik Z, Karaca K, Tuncayengin A, Karaoğlan U, et al.Extracorporeal shock wave lithotripsy for lower calyceal calculi. Eur Urol 1998;34:203-6.
23. Sakamoto W, Kishimoto T, Takegaki Y, Sugimoto T, Wada S, Yamamoto K, et al. Stone fragility –measurement of stone mineral content by dual photon absorptionmetry.
Eur Urol 1991;20:150-3.
IJSER © 2012
International Journal of Scientific & Engineering Research, Volume 3, Issue 11, November-2012
ISSN 2229-5518
31. Knapp R, Frauscher F, Helweg G, zur Nedden D, Strasser H, Janetschek G, et al. Age-related changes in resistive index following extracorporeal shock wave lithotripsy. J Urol
1995;154:955-8.
Shock wave lithotripsy 2: Urinary and biliary lithotripsy. New
York: Plenum Press; 1989. p. 3-6.
ESWL and blood pressure. J Urol 1995;154:2-4.
1994;25:99-104.
41. Shigeta M, Kasaoka Y, Yasumoto H, Inoue K, Usui T, Hayashi M, et al.Fate of residual fragment after successful extracorporeal shock wave lithotripsy. Int J Urol 1999;6:169-72.
44. Cicerello E, Merlo F, Gambaro G, Maccatrozzo L, Fandella A, Baggio B, et al. Effect of alkaline citrate therapy on clearance of residual stone fragments after extracorporeal shock wave lithotripsy in sterile calcium and infection nephrolithiasis patients. J Urol 1994;151:5-9.
1993;7:465-7.
48. Orestona F, Caronia N, Gallo G, et al. Functional aspects of the kidney after shock wave lithotripsy. In: Lingeman JE, Newman DM, editors.Shock wave lithotripsy 2: Urinary and biliary lithotripsy. New York:Plenum Press; 1989. p. 15-7.
49. Bierkens AF, Hendrikx AJ, de Kort VJ, de Reyke T, Bruynen CA, Bouve ER, et al. Efficacy of second generation lithotripters: A multicenter comparative study of 2206 extra corporeal shock wave lithotripsy treatment with the Siemens Lithostar, Dornier HM4, Wolf Piezolith 2300, Direx Tripter X-1, and Breakstone Lithotripters. J Urol 1992;148:1052-6.
Smith AD,Badian DH, Clayman RV, editors. Smith’s Text
IJSER © 2012