Department Of General Surgery of Advanced Medicare and
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 1
ISSN 2229-5518
A Comparative clinical Study on Open
Appendicectomy & Laparoscopic Appendicectomy
Shree Rajkumar Saha
Abstract-Appendicectomy is one of the most commonly performed surgeries worldwide. As it was commonly done by conventional open method but with the gradual advancement of more and more laparoscopic surgical procedures laparoscopic appendectomy is also p racticed now a day.
Methods: Total of 86 patients were selected initially for the study and 6 patients were excluded. Out of 80 patients 40 were in the open group and 40 were in the laparoscopy group.
Index term--Abscess, After8, After16, After24, After 48, Collection, Collection Problem, Ceal.Leak, Cosmesis Scar, Delay Healing, Disruption, DtOTTime, Gamma distribution, , G.I.Obstruction, IleusPost, Indoor Work, Likelihood, Lognormal distribution, LNGD, Or, Outdoor Work, , Retention, Stay Days, Surgery, , Transition Matrix. UTI, Vomating, Weibull distribution, WoundAbcess.
----------------------------------------------------------------------
ppendicectomy is one of the most commonly performed surgeries worldwide. It is commonly done
by conventional open method but with the gradual advancement of more and more laparoscopic surgical procedures laparoscopic appendectomy is also practiced nowadays. However, it has not yet been established which procedure is the gold standard.
The aim of this study is to compare the outcomes of these
two surgical procedures on different aspects and to find out any significant statistical difference between them. Age and sex factors were kept almost identical. Comparison was done on the basis of –operative time, post op. pain control, postoperative complications(wound, infective, urinary, pulmonary, g.i.t),post op. stay in the hospital, cost of surgery, time to return to indoor and outdoor activity, satisfaction with cosmesis and other complications if any.
This Prospective observational study was performed in the
Department Of General Surgery of Advanced Medicare and![]()
Shree Rajkumar Saha is currently guest lecturer in Achary Jagadish
Chandra Bose College affiliated to Calcutta University and N.C.T.E.,
1/1b,A.J.C.B.Road, Kolkata700020.WestBengal,India.www.ajcbosecollege.org.E-mail:
rajjuku@gmail.com, PH-00919836537236.
Research Institute (AMRI Hospitals), P-4and5, C. I.T. Scheme- LXXII, Block – A, Gariahat Road (Beside Dhakuria Bridge), Kolkata – 700 029, West Bengal between 1/2/2007 to
31/1/2010.
excluded out of study –
a) Children below 10 yrs of age
b) Suspicion of peritonitis of reasons other than appendicitis.
c) Diseases of appendix other than appendicitis.
d) All types of incidental appendicectomy. e) Previous pelvic surgery.
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 2
ISSN 2229-5518
Symptoms Score
Migration of pain to RIF 1
Anorexia 1
Nausea, vomiting 1
Signs
Lab
Tenderness (RIF) 2
Rebound tenderness 1
Elevated temperature 1
Leucocytosis. 2
Shift to left 1
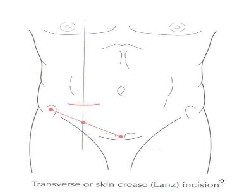
Fig.1.2 LANZ incision – transverse skin crease incision, appropriate
Total 10
A score of 7 is strongly predictive of acute appendicitis. Those patients with equivocal score (5-6) ,special
investigations – abdominal USG/CECT is done to avoid negative appendicectomy.
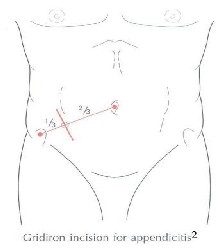
Fig. 1.1 Gridiron incision: (Gridiron: a frame of cross beams to support a ship during repairs. The incision is made at M.B point at right angles to a line joining the Rt. Anterior superior iliac spine to the umbilicus2
to the size and obesity of the patient is made approximately 2 cm below the umbilicus centered on mid cliavicular midninguinal line. In this incision exposure is better and if necessary may be extended medially by retraction or division of the rectus abdominals muscles.2
Patients asked to evacuate the bladder just before entering into operation theatre.
Position of Patient–Supine.
I.V.drip on Rt .Hand and extension used for i.v access by anesthetist at the time of surgery.
Left arm – by the side of the patient and kept in position with the help of a folded drape surrounding it and the ends placed under the chest.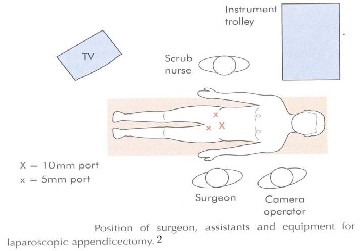
Figure 2
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 3
ISSN 2229-5518
During this study period both group of patients (open and laparoscopic appendicectomy) were observed for the following items for comparative study and analysis at the end of the study:
Time taken from starting of skin incision to the final closure
of the skin wound.
Here only operation theatre cost was considered which included anesthetic drugs, iv fluids, antibiotics, gas used for Laparoscopy, instruments and other consumable charges.
International Association for the study of Pain has described pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.41So pain is a subjective complaint and there is no definitive marker to measure the intensity of pain by patients. So, different methods for pain assessment e.g., McGill Pain
Questionnaire, Memorial Pain Assessment Card (MPA) etc. are in use world wide. Among these MPAC consists of three 100 mm visual analogue scales -pain scale, Relief scale, Mood scale and one with diff. adjectives of pain (e.g. Mild, moderate, severe etc.)
Of these 4, one -Pain scale was used in our study for the assessment of severity of pain.
In Pain V.A. scale – a 100 mm long line marked with least possible pain to the left end and worst possible pain marked at the right end was produced to the patient and asked them to mark of his/her own on the unscratched scale as per his/her own feeling of pain intensity at that moment and the score measured in millimeter from the left end of the line up to the mark given by the patient. and this scale was used for assessment of pain at 8hr interval in First 24 hrs and then at the end of 48 hrs. Analgesics were used as per necessity of the situation. This assessment of pain intensity was done routinely at the ward once patients were fully awake, the effect of anesthetic agents was over and patients could tell about their pain experience
Least Possible Pain ![]() Worst Possible Pain
Worst Possible Pain
0 50 100
.
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 4
ISSN 2229-5518
Here post operative complications were assessed as –
(i) Wound hematoma, seroma or persistent discharge. (ii) Delayed wound healing
(iii) Wound disruption
(i)Postoperative intraperitoneal abscess/subdiphragmatic abscess or collection
(ii) Post operative septic wound complication![]()
It has been calculated from the date of surgery to the date of discharge.
it is defined as return to usual work of domestic and social life at the discretion of the patient. It was assessed as follows:
a. When patients are fully mobilized. b. Able to perform their daily house
hold activities e.g. Maintenance of
personal hygiene, self dress up without assistance and able to go to toilet without help and can take food normally.
c. Good condition of operation wound d. No fever.
e. Pain sensation is minimal.
(i) Urinary retention.
(ii) Urinary tract infection.
(i) Post operative ileus.
ii) Post operative Small gut obstruction. iii) Nausea, vomiting
(iv Cecal / stump leakage.
![]()
Patients were followed up at OPD after 1st and 2nd week and were assessed as below:
a) Cosmesis of wound scar
b) Return to both house hold work and outdoor / office work.
c) Further complications if any.
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 5
ISSN 2229-5518
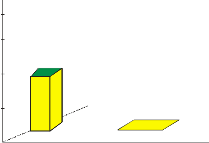
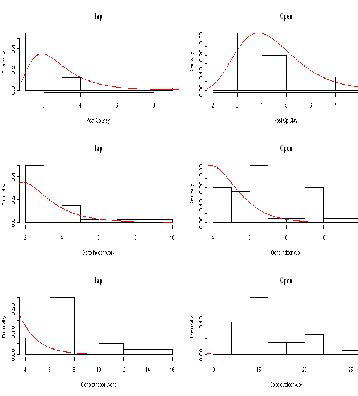
T ime for Lap Appendectomy(LA) n = 40
![]()
In the open appendectomy group out of 40 patients, 25 were female and 15 were male. In the Laparoscopic appendectomy group also there were 25 female and 15 male patients. Applying Chi-square test, p-value = 1.00. Thus sex ratios of the two groups do not differ significantly.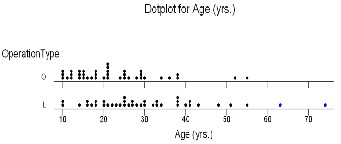
Regarding age distribution of the patients in both the study groups, applying Mood Median Test the age distributions were found to be significantly similar at 1% level of significance. Graphically we can also see it as follows:
Fig 3.
Patients serial
T ime for Open Appendectomy(OA) n = 40
![]()
Patients serial
Fig 4.The median value for operating time in open group was 35 mins. (range 15-60 minutes) and for Laparoscopic group it was 42.5 mins (range 20-120) with a p-value = 0.004. and thus operating time in LA group was significantly higher than that in OA group.
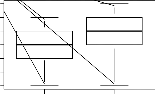
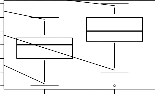
The following are the box-plots and line diagrams of assed pains after 8, 16, 24 and 48 hours corresponding to the two operation methods.
Thus keeping the age and sex factors similar we studied and compared our observations in both the groups on the following criteria.
The following figures show the operation times of the patients:
Assessment of pain at 8hr interval
lap open
Assessment of pain at 16hr interval
lap open
operation type
operation type
Assessment of pain at 24hr interval
lap open
Assessment of pain at48hr interval
lap open
operation type
operation type
Figure 5. We observe mean and quartile pain in 8hrs,16h,24h to be less in case of LAP surgery, but in 48h mean pain is less and 3rd quartile pain is lower in case of OPEN surgery.
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 6
ISSN 2229-5518
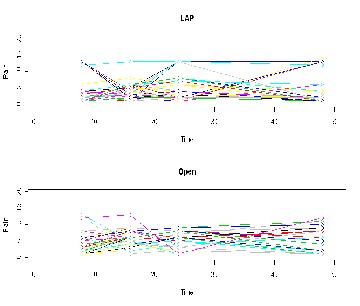
Fig 6.: It is not clear whether there is the
significant change of pain with respect to time.
5.2 Longitudinal analysis of pain : Parametric model
we may consider the Longitudinal(LNGD) study for different timepoints of pain for the both groups of patients. So here
we assume three LNGD model:
1.Painij =a+ai +b(j)+q(surgery=open)+eij
where, a :N(0,s2 ),e :N(0,s2 ) ; , i=person in the treatment
b=time coefficient(parameter); j=8,16,24,48;
2. Painij =a+ai +g j +q(surgery=open)+eij
where, a :N(0,s2 ),e :N(0,s2 ) ; , i=person in the treatment
g j =jth time factor ; j=8,16,24,48;
3.Painij =a+ai +q(surgery=open)+eij
where, a :N(0,σ 2 ),e :N(0,σ 2 ) ; , i=person in the treatment
i a ij e
j=8,16,24, 48
We obtain the following results from analyzing the three models:
TABLE 1.Analysis of model -1
Fixed | Value | Std.Error | DF | t-value | p-value |
effect(intercept | |||||
(Intercept) | 4.194 | 0.535 | 239 | 7.841 | 0.000 |
Surgeryopen | 1.025 | 0.490 | 78 | 2.091 | 0.040 |
timepts | 0.195 | 0.163 | 239 | 1.197 | 0.233 |
![]()
TABLE 2 .Model-2 estimated values and std.error, p-value as follow
Fixedeffect(intercept) Value Std.Error DF t-
value
p-value
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 7
ISSN 2229-5518
TABLE 3 .Model-3 estimated values and std.error, p- value as follow
Intercept (3.146, 5.242)
Value Std.Error DF t-value p-value
(Intercept) 4.681 0.347 240 0.347 0.000 surgeryopen 1.025 0.490 78 2.090 0.040
Model 2 surgeryopen (0.064 , 1.986) 1721.851 1748.119
Intercept (3.355, 5.195)
Model 3 surgeryopen (0.064 , 1.986) 1718.558 1733.607
Intercept (4.002 , 5.361)
TABLE- 4 Confidence interval and AIC of three models
lap (individually) open(individually)
a b c a b c
Comments: Here model- 3 is the best model because no significant time point effect or time factor effect (considering model-1 and
The no. and duration of use of analgesics (injection and oral) were observed lower in the Laparaoscopic group in comparison to open conventional method. So, LA group patients suffered less post operative pain than OA group which was statistically significant (p-value =0.039)
b 0 19 12
c 0 0 1
b 0 7 12
c 0 1 17
6.1 WOUND
1.Pain transition 8th h to16th h a=minor,b=middle, c=severe
a b c a b c
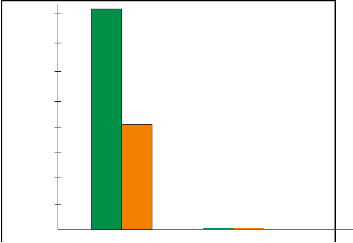
In this study 4 cases of serious collection in wound were seen in open appendectomy group and two of them later showed sign of infection. They were managed by conservative method and with daily
a 1 0 0
b 4 20 1
a 0 1 1
b 0 6 4
dressing.
TABLE -5 In Lap group – no such collection was seen.
c 1 7 6
c 0 2 26
Open n=40 LAP n =
P Value
2.Pain transition 16th h to 24th h a=minor,b=middle, c=severe
a b c a b c
Collection in wound
4 (10%)
40
Nil
0.018
a 4 2 0
b 5 21 1
c 1 5 1
a 0 0 0
b 1 5 3
c 0 12 19
Infection in wound
2 Nil
3.Pain transition 24th h to 48th h a=minor,b=middle, c=severe
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 8
ISSN 2229-5518
4
3.5
3
2.5
Type of Surgical Procedure
Fig-7 Bar chart showing number of patients with wound in the two surgical methods
Thus at 5% level of significance collection in wound is significantly low in Lap. Group than in O.A. group
2
1.5
1
.5
0
OPEN LAP
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy
9
ISSN 2229-5518
In this study 3 cases of delayed wound healing were noted in the open appendectomy group – out of them 2 were associated with wound collection and subsequent infection and managed conservatively and 1 case was associated 1 only serious collection in the wound.
In Lap group no such delay in wound healing could be seen. TABLE 6
6.2.1Intra peritoneal collections
In Laparoscopic group 3 patients had intraperitoneal collections who subsequently underwent serial USG and was under conservative treatment. None of them required active interventions. No case of intraperitoneal abscess was found.
In contrast – no case of intraperitoneal collection or abscess was found in open group.
Open
(n=40)
LAP
(n=40) p- value
TABLE 7
Nil
0.036
Open Appen (n=40)
LAPAppendecto
(n=40)
(7.5%)
Nil 3
(7.5%)
0.036
Fig-8 Bar chart showing number of patients with delay in wound in the two surgical methods
Fig-9 Bar chart showing number of patients with delay in
4 Intraperitoneal Collection in the two surgical methods
3.5
3
2.5
2
1.5
1
.5
OPEN
0
Collection + Infection
Collection
LAP
4
3.5
3
2.5
2
L
1.5 A
1 P
.5
OPEN
Type of Procedure
Thus as 5% level of significance delay in wound healing is significantly lower in Lap – Appendicectomy group than in O.A.
No case of wound disruption was found in either study group.
0
Type of Procedure
Thus at 5% level of Significance Post operative intraregional collection / abscess formation is significantly higher in LA group than OA group.
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy
10
ISSN 2229-5518
In this study group – no wound infection was noted in the lap group.
TABLE 9
Open n=40 LAP n = 40 P
In open group – 3 patients had wound infections.
TABLE 8
5%
1
2.5%
0.555
Open Appendictory (OA)
(n=40)
LAP Appendictomy (LA)
(n=40)
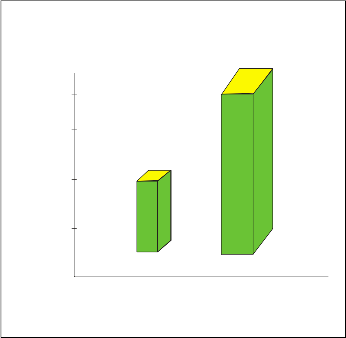
Fig. 11Bar chart showing number of patients with Retention of Urine surgical methods
3
7.5%
Nil P=0.036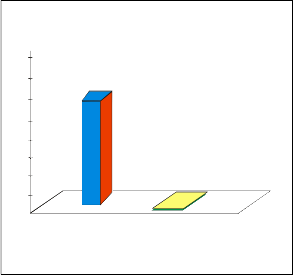
2
Fig. 10 showing number of patients with wound in the two surgical methods
4
1.5
1
3.5
3
2.5 O P
2 E
1.5 N
.05
0 OPEN LAP
1 n=40
.5
0
L A P
Type of Procedure
Type of Surgical Procedure
Thus at 5% level of significant post O.P. wound infection is significantly low in LA group then OA group.
6.3.1Retention of Urine
Thus there is no significance statistical difference regarding post operative retention of urine in either group.
TABLE 10
In our study one case of UTI was found in OA group and none in LA
group p value = 0.311
In our study two cases of post op. urinary retention in OA group and one in LA group happened which needed catheterization for bladder evacuation.
Observied value
for
UTI
OA
n=40
1 (2.5%)
LAP
n = 40
0
-
0.311
Fig.
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy
11
ISSN 2229-5518
Ffig 12-Bar chart showing number of patients with
UTI in the two surgical methods
Fig Fig. 13 Bar chart showing number of patients wit iting in the two surgical methods
2
1.5
1
.05
0
OA
LA
Type of Procedure
7
6
5
4
L
3 P A
2 E P
1 N
0
Thus there was no significant difference in rate of UTI
found in either group.
No cases of chest infection or any other chest complications were noted in either study group.
In this study group 5 patients were found to have post operative Nausea and vomiting in open method.
In laparoscopy 6 patients had increased nausea and vomiting.
All of then were managed by IV-fluid, injection antiemetic and had delay in taking oral feed.
TABLE 11
Type of Procedure
So there is no significant statistical difference in
Nausea and Vomiting observed in either group.
6.6 ILEUS
In our observation we found one patient developing post operative Ileus in open appendectomy method. In contrast there were 5 patients who had developed post operative Ileus. All these cases were managed by iv. fluids, delay in oral intake of food and other conservative treatment None of them required any active interventions.
TABLE 12
Open n=40
5
12.5%
LAP n =
40
6
15%
0.745
Open
(n=40)
1 (2.5%)
LAP (n=40)
5 (12.5%)
0.042
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy
12
ISSN 2229-5518
Fig. 14 Bar chart showing number of patients with
ILEUS in the two surgical methods
5
6.7 Gut Obstruction
In Laparoscopy group one case of post operative gut obstruction was observed which was managed conservative. In OA group no case of gut obstruction could be seen.
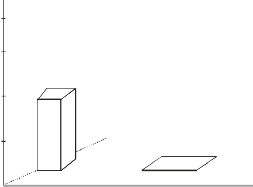
TABLE 13
Open
4 n=40
LAp n =
40
3 Postop Gut
L obstruction
2 A
P
1
2.5%
Nil 0.311
1
O
P E N
0
Type of Procedure
Thus at 5% level of significance rate of post Operative Ileus is significantly more in LA group than OA group.
Fig. 16 Bar chart showing number of
patients Gut Obstruction in the two surgical methods
2
1.5
1
Open 2.5%
LAP
12.5%
.05
0
OA
LA
Type of Procedure
Thus there was no statistical significant difference regarding post op. Gut obstruction in both the groups.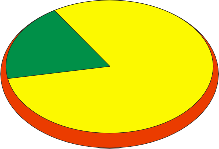
Fig. 15 Pie Chart Showing Rate of Post
Operative Ileus.
7 Total duration of stay in the hospital from the date of operation
7.1 Model based analysis
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 13
ISSN 2229-5518
x
![]()
f x k xk 1 e
![]()
; , for x 0; and k, 0 1
k k
where k> 0 : the shape parameter, >0 :the scale parameter, x =day i
x k
k x k 1
![]()
![]()
f x;7k.2,E stimation ofepa rame, txerw0 ith likelihood m2 ethod
we finaly decided to use the lognormal model .
Here
0 ,
x 0
We estimstethe parameter with likelihood estimation technique
whaenredkc>he0c:kthteheshacpoenspiasrtaemnceytewr, ith>0he:tlhpeosfcasleimpaurlaamtioetnert,excih=ndiaqyue.
Hence required formula as2follows:
1 ln x n 1
1 L 2 x i N
![]()
![]()
![]()
we observe that f (x;m,s)= f (lnx;m,s)
f x; ,
e i=1
, 0
3
![]()
and here we get solution after differentiating w.r.t , m, s ,and
x 2
Ù
where and lnxare theparlanmx e-tμers hence x =days
k
![]()
Angdept;imck=-ukp best,osn2 =e wk ith helpof t.he AIC, where
AICfo=r2ke-q2u(llni(Ln)L),awphe&reokpistnhe .nro.t odfapyasramers &
ty en w
L is the maximu^m va^lue ^of m^le.
we have,H01:μ1i = μ2i ,σ1i = σ 2i ;i=1,2,3
The test statistic is
=-2(ln(likelihood for null model)-ln(likelihood for
D
alternative model))
![]()
=-2ln
likelihood for null model
. which follows χ 2
Probe dens model
TABLE 14
Operation type AIC (stay s days )
AIC (indoor and out door days)
comment s
likelihood for alternative model
with d.f
Gamma Lap Appendectomy(LA)
n=40
6.909 10.329 Not significa
nt
OpenAppendectomy
(OA) ,n = 40
6.286 11.390
Weibull Lap Appendectomy (LA)
n=40
6.800 8.898 Less significa
nt
OpenAppendectomy
(OA) ,n = 40
6.709 9.308
Log- Normal
Lap Appendectomy (LA)
n=40
6.104 8.183 Signific ant
respect than
(OA) ,n = 40 6.256 9.018
other two
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 14
ISSN 2229-5518
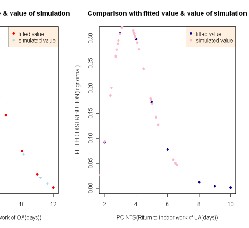
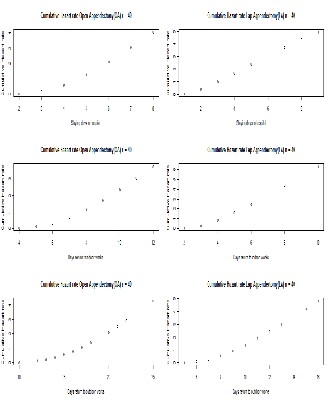
Comparison with fitted value & value of simulation
fitted value simulated value
2 3 4 5 6 7 8
Comparison with fitted value & value of simulation
fitted value simulated value
2 4 6 8
POINTS(post stay days of OA)
POINTS(post stay days of LA)
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy
15
ISSN 2229-5518
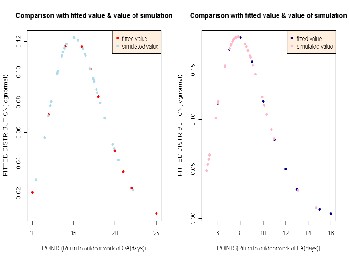
the time to return to normal indoor life was statistically significantly lower in LA group than in OA group.
Return to outdoor Work –
In this study the Patients underwent open appendectomy
Fig. 17
returned to outdoor works with a median of 15 days from
Table 15 Estimated parameters and the conOsepqeureanticoen
of date (range 10-25) whereas in the
likelihood ratio test
Return to normal indoor activity –
Laparoscopy group it was only 8 (range 5-16). As such, the
Laparoscopy group enjoyed the freedom of early return to
outdoor work significantly earlier than the Open group.
So, Pt’s who underwent Lap-appendicectomy started daily
routine indoor activities much earlier than the Open group and![]()
variable | Type | Average | T- | T- | P-value | Differenc | Confiden |
surgery | cost | value | tabulate | e of two | ce | ||
d value | mean(D) | interval | |||||
with 78 | of D | ||||||
df | |||||||
Cost | open | 8515.0 | 1.665 | 0.039 | 7047.5 | (368.78, | |
Lap | 15562.5 | 2.129 | 13726.21 ) | ||||
Log(cost | open | 8.980 | 3.974 | 1.665 | 0.000 | 0.431 | (0.214, |
) | lap | 9.411 | 0.647) |
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 16
ISSN 2229-5518
TABLE 16
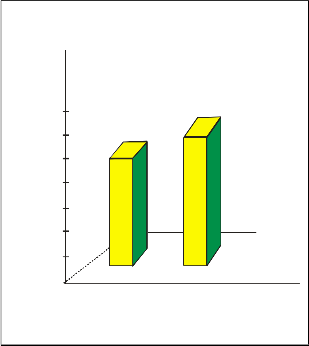
Comments: In Open Group we found mean cost of Operative procedure of Rs. 8515/- and in Laparoscopy group it was Rs.
15562.5/- and P value = 0.039 and calculated t-value is greater i.e. statistically very significantly high in Laparoscopy group over Open group at 5% level.
Regarding cosmesis the VAS was used and the value on the lower side of scale indicating better result of cosmesis of scar and Patients observation was noted. The median value for open group was 2 [ range 1-6] and that for Lap Group was 1 [0-3].
TABLE 17
Kruskal-Wallis Test: Cosmesis versus OperationType
Kruskal-Wallis Test on Cosmesis
Operatio N Median Ave Rank Z L 40 1.000 32.8 - 2.97
Fig. 18 It is clear from the figures that patients undergoing LAP need less time to return to normal life than those undergoing OPA
8.1Graphical analysis:
1. Mean cost (Including outlier)
O 40 2.000 48.2 2.97
Overall 80 40.5
H = 8.84 DF = 1 P = 0.003
H = 10.46 DF = 1 P = 0.001 (adjusted for ties)
TABLE 18
Open n=40 LAP n = 40 P Value
2. Mean cost (Excluding outlier)
2
[1-6]
1
[0-3]
=0.001
lap vs open

lap open
2
1.5
operation type

lap vs open
1
.05
O P
E L
N A P
lap open
0
Fig. 20 Type of procedure
operation type
Fig. 19
Here for comparing the cost ,we use the t test with given cost
of surgery both Open and lap and taking log transformation of cost.
we also perform same test (after removing skewness )of data, the
cosequence as follows:
our null hypo is, H0 : 1 2
IJSER © 2012
The research paper published by IJSER journal is about A Comparative clinical Study on Open Appendicectomy & Laparoscopic Appendicectomy 17
ISSN 2229-5518
So, Laparoscopic group had better satisfaction with cosmesis and the difference was statistically significant (P = .001)
No other complications could be seen in any group.![]()
Here we consider two type of operation technique - one is Laparoscopic Appendicectomy (LAP) and the other Open Appendicectomy(OA) . Here we analysis the data graphically, also apply some statistical test. And here important analysis is fitting data with some standard probability model and longitudinal analysis and hazard rate analysis.
Age: With help of dot plot we see that we get 60+ patients in
LAP.
Time required for surgery: From the bar diagram we see that more time is needed in LAP.
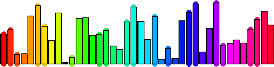
Cost of surgery: We see need more cost in LAP with Histogram. Also, performing the t-test we find significant difference in the two costs.
Pain: Graphically, from box plots and line diagrams, it is not clear how pain varies with time in the two surgical methods. However, from the transition matrix this variation is quite clear. Also fitting the longitudinal model we get better significant relation between pain and surgical method.. Here LAP gives better result.
Post operation stay, Going to indoor work and Going to outdoor work: Here we get better fitted model is lognormal model and performing the likelihood ratio test between the two surgery procedure In every case we may reject the null hypothesis that that post operation stay days and others days for OA and LAP differ significantly. Hazard analysis we also get the require remedy’s days is less in case of LAP.
From the present study it has been observed that appendectomy done either by open method or laparoscopically is comparable in terms of operation time, post operative pain control, post operative Complication, post operative stay, convalescence, cost and cosmesis.
Where OA(open appendicectomy) was associated with less operative time, less cost and less chance of post operative Intra Peritoneal collection and ileus in one hand, it had got disadvantages like more post operative pain sensation, more number of analgesic used, more incidence of operative wound collection, delay in wound healing, more stay in hospital and delay to start oral feeding and return to normal life.
On the other hand LA(lap appendicectomy) was associated with more operative time, increased operative cost and more incidences of intra-peritoneal collection and ileus but there are advantages like less pain sensation, less requirement of analgesics, less wound complications, less hospital stay and earlier introduction of oral feeding and quicker return to normal life.
So finally we conclude from our study that laparoscopic appendicectomy is not only comparable to conventional open method in regards to feasibility and safety but also with more and more successful use of it, one day it may be the gold standard approach in treating a case of acute appendicitis in near future.
Acknowledgment
I wish to thank Professor Manisha Pal, Dr. B. Ganguly Professor S. Sengupta, Professor U. Bandyopadhyay, Professor. S. Senroy and Dr. Goutam Gosh. This work was supported in part by Department of Statistics, University of Calcutta.
References
[1].RUPERT G.MILLER,JR. ,GAIL GONG,ALVARO MUNOZ
(1981):Survival Analysis. Wiley-Interscience Publication, John Wiley and Sons.Inc,USA
[2].PETER J.DIGGLE, PETRICK J.HEAGERTY, KUNG-YEE LIANG and SCOTT L. ZEGER(2001): Analysis of Longitudinal Data, Washington, OXFORD university press.
[3] JOHN P. KLEIN, MELVIN L. MOSCHBERGER (1997): Survival
Analysis Techniques for Censored and Truncated Data. Springer-Verlag New York,Inc.
[4].ANUP DEWANJI, KRISNA S.GANGULY, PARTH P.MOHANTO, TAPAS SAMANTA AND BIKAS K.SINHA.(2002). A Study of Pulsed Electro-Magnetic Field Therapy for Rheumatoid Arthritis patients : Analysis of Adjustment Period Data, Calcutta Statistical Association Bulletin, Vol. 53, Nos.211-212, pp
R, Minitab, SPSS, Microsoft Excel.
IJSER © 2012